So far, Minnesota Governor Tim Walz has largely been a responsive caretaker governor, responding to the crises du jour rather than than actively pushing a progressive agenda and building a legacy for himself.
Governor Walz’s legacy is essentially “pissed off all sides while consumed with thankless pandemic management.” I think he did a reasonably good job managing the pandemic, but he definitely had to make enemies doing it.

One partial break from caretaker mode was his poorly named “ONECare” proposal, which would give Minnesotans the option to buy into MinnesotaCare. MinnesotaCare is a longstanding program serving low-income individuals and families who can’t get employee-sponsored health insurance and don’t quality for Medicaid, which is called Medical Assistance (MA) in Minnesota.
Giving Minnesota health insurance consumers of all income levels this additional option would ensure that every Minnesotan in every county had at least one health insurance option available to them. That’s a big deal. It also would bring more competition to an individual market that sorely needs more competition. Over time, this could result in lower premiums for consumers.
Walz has not pushed his proposal particularly hard. Meanwhile, other states’ Governors are leading their states forward.
Colorado and Nevada this year passed public option plans—government-run health insurance plans—that are set to launch in 2023 and 2026, respectively. They join Washington state, which enacted its law in 2019 and went live with its public option in January.
The early results from Washington state’s experiment are disappointing. In many parts of the state, premiums for the public option plans cost more than premiums for comparable commercial plans.
Many of the state’s hospitals have refused to take part in the public option, prompting lawmakers to introduce more legislation this year to force participation if there aren’t sufficient health insurance options in a geographic area. And consumer buy-in is also meager. In its first year of operation, the state health insurance exchange sold only 1,443 public option plans, representing fewer than 1% of all exchange policies.
Michael Marchand, chief marketing officer for the Washington Health Benefit Exchange, the state’s health insurance marketplace, said it’s premature to judge the program by its first year.
During the earlier years of Obamacare, the premiums for many commercial plans were high, he pointed out. Eventually, as insurers became more knowledgeable about the markets, prices dropped, he said.
If Governor Walz would get re-engaged in this issue and actively market his plan, they could learn from the experiences of Washington and avoid it’s mistakes. For instance, in areas where there is insufficient health insurance competition, Walz could require hospitals to participate.
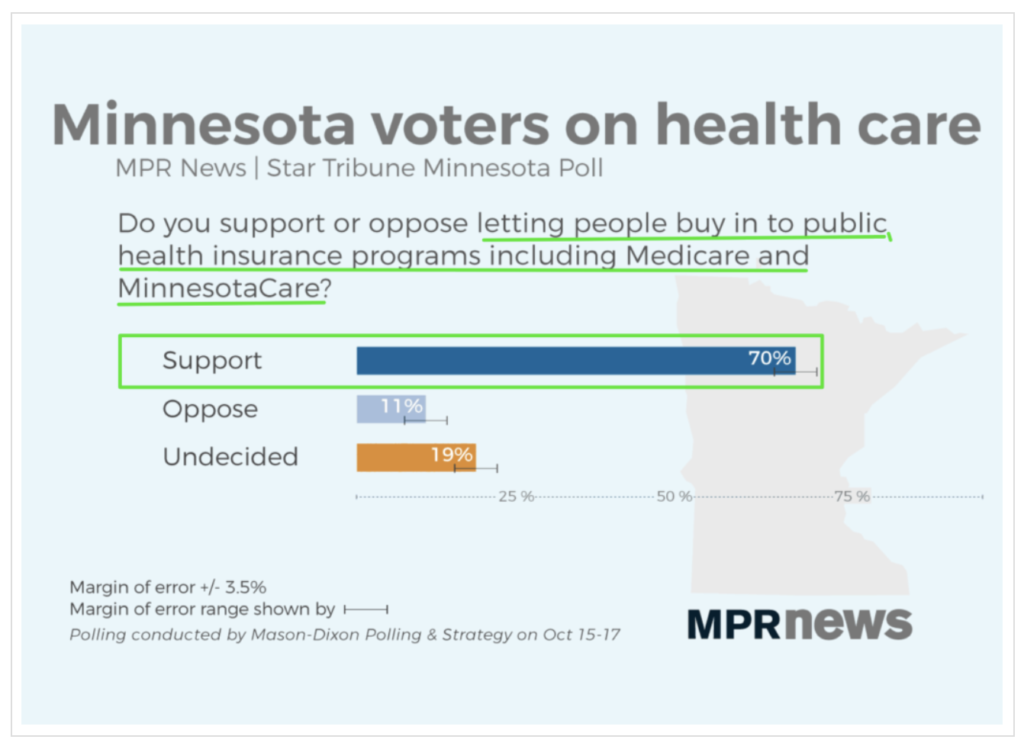
A MinnesotaCare buy-in option is extremely popular — only 11% oppose it, according to a Minnesota Public Radio survey. This is probably in part because it is an option. Any Minnesotan who opposes buying into MinnesotaCare — because of conservative ideology or because MinnesotaCare turns out to be expensive or poor quality — they can vote with their feet, as consumers in the state of Washington are doing.
Fighting for a MinnesotaCare buy-in option makes sense for Walz. The polls consistently show that health care is a top issue for voters, and huge majorities consistently trust Democrats over Republicans on that issue.
Moreover, in the 2022 gubernatorial general election campaign Walz may very well be running against a physician, Scott Jensen. This will ensure that health care is high profile in the race. Therefore, candidate Walz needs to be seen fighting for better health care, and this proposal gives him that platform.
If a MinnesotaCare buy-in option passes, Walz finally has a legacy beyond pandemic management. If Senate Republicans kill it, which seems likely, Walz has a great political argument to make while running for reelection and trying to retake the Senate: “I worked my ass off to give you another health insurance option and bring you some price competition, but Republicans like Scott Jensen opposed it on orders from private insurance lobbyists. If you want to more options and more price competition, vote for me and change the Senate leadership.”
Pushing a public option is a great political option for Walz. So why is he so damn cautious about it?